Ophthalmology Department
Download the leaflet
Eyelid Ptosis Surgery (317kB pdf)
Introduction
This leaflet is for parents / caregivers of children undergoing ptosis surgery for droopy eyelids.
What is Eyelid Ptosis?
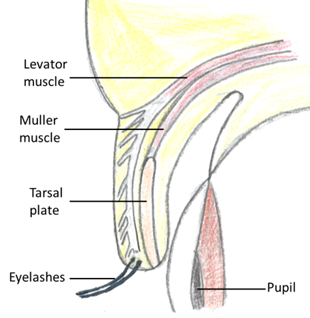
Eyelid ptosis is a drooping of the upper eyelid. There are two muscles that lift the eyelid up: Levator Palpebral Superioris (the main muscle, also referred to as levator) and Muller’s muscle (the accessory muscle).
A ptosis usually develops because of a weakness in the levator muscle itself, weakness to nerve supplying the muscle or the way it has developed. Occasionally there may be a weakness in the Muller’s muscle.
It may also be caused by the muscle separating from its surrounding support. A few reasons for this include injury, long term contact lens wear or previous eye surgery.
The ptosis, depending on its extent, may affect the vision and visual development, especially in children below the age of 7. You may notice that your child is raising their eyebrows and chin to lift the eyelids. This may in turn cause tiredness of the forehead muscles or ache in the neck due to adopting this posture.
What is eyelid ptosis surgery?
Ptosis surgery is an operation to raise the upper eyelid. There are several different procedures, which we have described below. Your surgeon will tell you and your child which one they will be having.
The choice of operation depends mainly on whether the problem was present since birth or whether it developed later in life, and how much the eyelid moves.
- Brow Suspension:
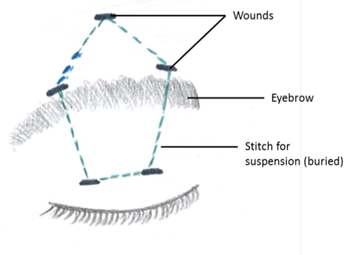
This is used in children in whom there is very little eyelid movement. People who are born with a ptosis (congenital) usually require this procedure. In congenital ptosis, the eyelid muscle (levator) has not developed properly, and so strengthening it with stitches does not work. A brow suspension procedure uses the forehead muscle (frontalis) to lift the eyelid.
This muscle causes us to have forehead lines and enables us to lift the eyebrow.
Using a non-absorbable material (such as prolene, silicone or fascia lata), the eyelid is connected to the forehead. The stitch is passed under the skin and eyebrow using five small openings, each less than ½ a centimetre long. Two of these openings are in the eyelid, two at the upper border of the eyebrow and one in the forehead.
- Levator Aponeurosis Advancement / Resection:
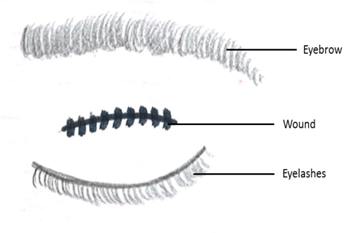
This procedure is used when the levator muscle has some, but not full, strength. For this procedure, an opening is made in the natural skin crease of the eyelid. The levator muscle is pulled forwards and strengthened with stitches.
Dissolvable stitches are then used to reform the natural skin crease in the eyelid, as well as close the opening. These stitches will fall out by themselves.
In some cases of congenital ptosis, a levator resection is done. In this case, a segment of the levator muscle is cut out and the muscle is advanced, in effect strengthening or tightening it. This is used when the muscle itself is weak.
- Muller’s Muscle Resection and Advancement:
This procedure is useful for small amounts of ptosis (e.g. 1-2mm). It involves approaching the Muller’s muscle from inside the eyelid, removing a part of it and then bringing forward to strengthen it. Deep stitches are used that do not need to be removed. There is no opening made in the skin itself.
What are the benefits of surgery?
These depend on the problems that the ptosis is causing to your child and may include:
- Lifting the eyelid so that it would be easier to see from that eye.
- In young children, if the ptosis is covering the pupil, there is a high chance of permanently limiting the development of vision in that eye (amblyopia). By lifting the eyelid we aim to improve stimulation of that eye and thus help vision development. We may need to consider other treatment after surgery, such as patching of one eye to encourage this. This will be discussed with you if it is relevant.
- Improving the cosmetic appearance by making the eyelids more symmetrical.
- Reducing the need to lift the eye brows or the chin, and thus reducing the tiredness or ache associated with this.
What will happen if we decide not to have the surgery?
In the case that the eyelid ptosis does not cover the pupil, this will not damage the eye in any way. The ptosis may stay the same or gradually get worse. We can always observe visual development and re-visit the decision in the future.
In the situation that the ptosis covers the pupil, we will have a discussion to ensure the surgery does take place. This is because if surgery does not occur, then there is a high risk of poor visual development, and hence amblyopia, in children below the age of 7.
Above the age of 7, and if there is good vision, there is no rush for a decision regarding surgery. We often involve the child in the decision making process at that stage.
What will happen before surgery?
Before the operation, your child will be seen in the clinic by your consultant or a member of the team.
The doctor will ask you about the problem, any other medical problems and any medications that your child takes.
The doctor will examine your child’s eyes and eyelids, with special emphasis on visual development. Your child might see an orthoptist (they are specialists in assessing vision and visual function) and an optometrist prior to making a surgical decision.
If you are to proceed with surgery, the operation will be discussed in detail. This will include any risks or possible complications of the operation. All procedures in children are performed under general anaesthesia.
You will be asked to read and sign a consent form after having the opportunity to ask any questions.
What are the risks and possible complications of surgery?
Common
Under-correction: The eyelid is not lifted enough and so more surgery may be required
Further surgery: Your surgeon will takegreat care to lift the eyelid by the correct amount. It is possible for the eyelid to be lifted too high or left too low. Both may be addressed by further surgery. The contour or curve of the eyelid may initially look abnormal. This is often due to swelling and will usually settle within 3 months. If not, further surgery can improve it.
Facial asymmetry: It is common for a slight difference between the two eyes to remain after ptosis surgery.
Scar: Whenever the skin is incised a scarmay form. Every attempt is made by the surgeon to minimise and hide scars, but sometimes they can be visible.
Uncommon
Overcorrection: The eyelid is lifted too much and so does not close completely. This can result in the cornea (front window of the eye) being exposed and so drying out. This could cause some irritation. However it can result in ulceration of the cornea, which can then become infected, and cause severe pain and reduced vision.
Infection: Might present as increased swelling and redness of the skin. There might also be yellow discharge from a wound. Infection is treated with antibiotics.
Bleeding: May present as fresh bloodoozing from the site of surgery or a lump appearing near the wound after the operation. Simple pressure on a skin wound is usually enough to control minor bleeding.
Rare
Loss of eye: If the cornea becomes infected, it can be difficult to treat and can eventually lead to loss of the eye due to severe pain and reduced vision. This is very rare.
Loss of vision: Blood maycollect in the orbit, behind the eye, and could compress the nerve of vision and threaten eyesight. It is extremely rare for this to occur. It presents as pain, loss of vision and forward bulging of the eyeball, and is an emergency. If not treated quickly, it can lead to permanent loss of vision. This is very rare.
What should I expect after surgery?
After surgery, your child may experience some pain. Simple paracetamol is usually enough to control this.
The eyelids may be bruised and swollen. Bruising will take up to 2 weeks to settle. Swelling is greatly reduced after 2 weeks but may not completely resolve for 3 months.
The eyelid height and contour may change over the first 3 months, after which final judgement of the result of surgery can be made.
As mentioned above, your child may need to start treatment to help improve the vision development of the eye. This may include wearing glasses as well as patching of one eye. This will be discussed prior to surgery
Instructions for after Ptosis Surgery
For 10 days, the wound should be cleaned using boiled water that has cooled down, and sterile cotton wool balls. Avoid getting soap over the wound or rubbing the eyes.
Cool compresses may be used if your child is uncomfortable or complains about their eyelid(s). It is recommended that these be done for 10 minutes, every hour, for 4 days.
At discharge from the hospital you will be given an antibiotic ointment (Chloramphenicol). This needs to be applied to:
- Skin wound(s), three times a day for 2 weeks.
- Operated eye once every hour whilst awake till reviewed in clinic
A follow up appointment will be scheduled for 1 week after the surgery. If there are any concerns, please get in touch with the secretary or clinic and we will arrange to see you as appropriate:
Hospital telephone number: 0151 228 4811
Extension for clinic: 2215
Extension for secretary: 2839 / 3595 / 2961
This leaflet only gives general information. You must always discuss the individual treatment of your child with the appropriate member of staff. Do not rely on this leaflet alone for information about your child’s treatment.
This information can be made available in other languages and formats if requested.
Alder Hey Children’s NHS Foundation Trust
Alder Hey
Eaton Road
Liverpool
L12 2AP
PIAG 258